




A wrist fracture treatment algorithm, after 10 years of presentations at congresses, was first published in the SICM Hand Surgery Journal in 2012. During the 10 years from 2002 to 2012 angular stability volar plate systems, which slowly evolved from the fixed angle to the polyaxial variable angle, became evident. What has changed in the past 8 years?
The CT scan which increasingly guides, in each classification system, the treatment of a wrist fracture with radiological signs of instability has been enhanced with new technologies such as the “cone beam” CT scan, from maxillofacial applications. CTCB is increasingly replacing traditional CT in anatomical districts such as the wrist and hand, and thanks to lower ionizing radiation emissions with higher and higher resolution, it can often replace traditional radiological scans when a bone impingement or a “gap” or an articular “step-off” or an evolving bone consolidation process must be better interpreted.
MRI with the new high-field machines (1.5 3T) remains the gold standard in the diagnosis of associated ligament injuries.
External fixators have maintained their niche role and have evolved with sterile disposable kits and increased assembly simplicity (only 1 tool to assemble all of the components).
The “spanning plate” (also called bridge plate or distraction plate or Internal Fixator), increasingly used in articular fractures with severe and marginal comminution and in polytrauma patients with bilateral fractures, has joined the rejuvenated External Fixator, and competes with this for offer greater stability with minimal joint distraction (the percentage of the known secondary algodystrophy is reduced) and to eliminate the problem of infection of the fisches especially when the consolidation process takes more than 3 months (osteoporotic bone of the elderly). However the choice is still a dependent surgeon strategy.
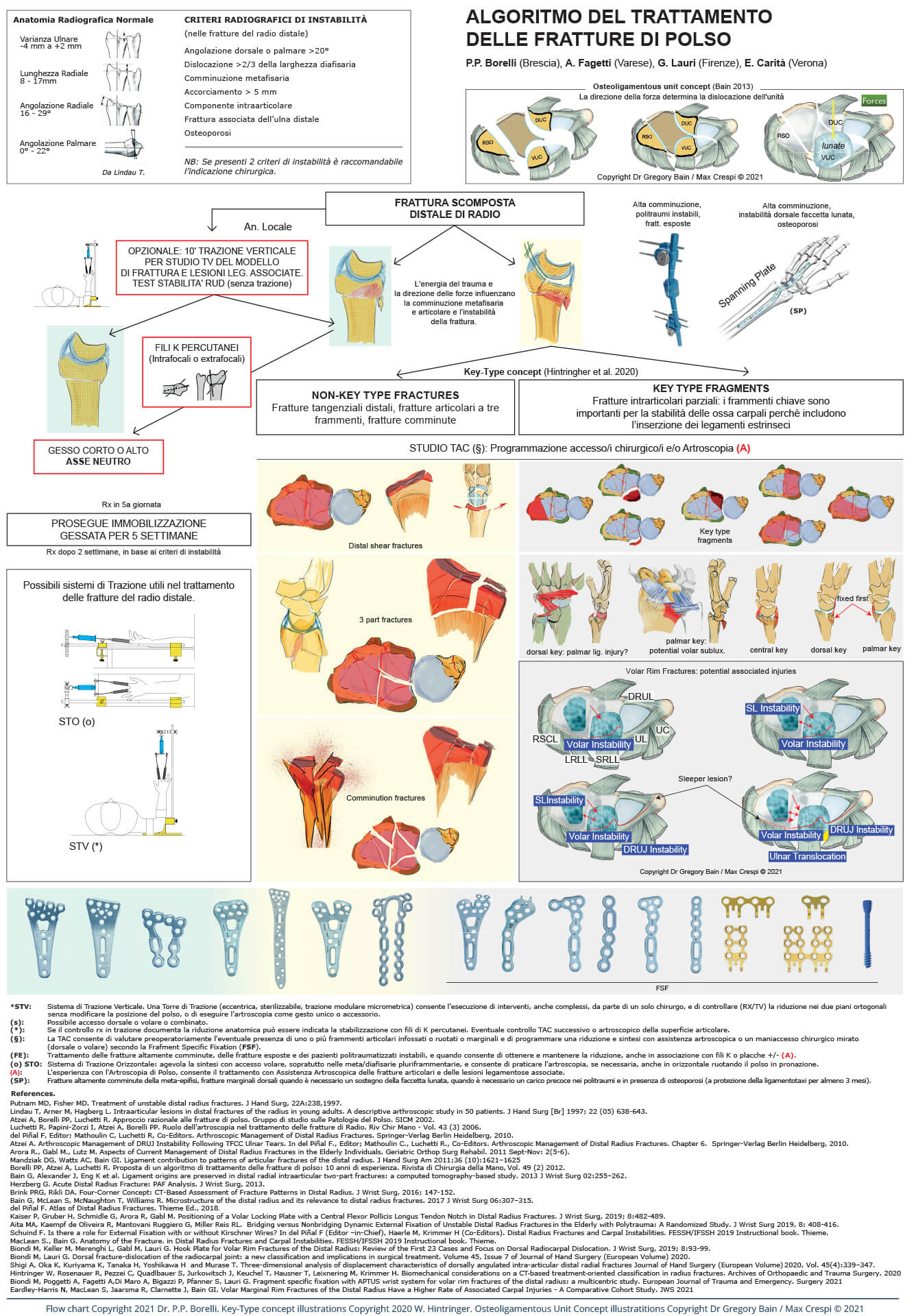
It is above all curious to note the return to FSF (Fragment Specific Fixation) which characterized the fixation of wrist fractures in the 90s, that is, increasingly focused on an anatomical stable reduction of single fragments with multiple surgical, volar, dorsal or combined approaches. In recent years surgical sets have gradually developed with plates of various shapes, with hooks incorporated at the distal end, and with “hook plates” increasingly dedicated to the variable sizes of marginal fragments or “key fragments” (fragments with ligament connections) or to those fragments that give stability to the entire assembly and therefore to the wrist as a whole. The market has turned towards a search for a fixation system as complete as possible to manage all the fragments of each size of a complex fracture in a stable way. The challenge is still open even if we have to recognize that some systems, including the one represented in the algorithm, have perhaps completed the “puzzle” of devices capable of addressing all the representation variables of distal radius and ulna fractures.
However, we must not forget the variable of associated ligament injuries which makes it more justified for a surgeon to deepen their experience in wrist arthroscopy. The argument is still controversial. There are in fact expert surgeons who do not consider arthroscopic application necessary for a good anatomical reduction and relative stable fixation of a wrist fracture and who rightly believe that an associated ligament injury may also be suspected by the particular direction of the fracture line on a standard x-ray and diagnosed with dynamic radiological examinations ( “stress view” under traction or dynamic fluoroscopy for the interosseous ligaments of the first row ), or with clinical tests (ballottement test for the TFCC complex ligament), tests performed preoperatively (traction stress view) or, more frequently, once fracture fixation has been performed.
However, it is necessary to recognize the role achieved by wrist arthroscopy in the treatment of wrist fractures, precisely for the evaluation of associated ligament injuries or superficial osteocartilaginous injuries, often not detected from standard x-rays. After suspecting it, it is important to “quantify” (remember the ability of spontaneous healing of most ligament injuries!) and possibly treat an associated ligament injury or highlight and remove a free “osteocartilage” body or partial detachment (site of a subsequent potential osteoarthritis), and/or to adapt the postoperative rehabilitation process to the necessary time required to heal the associated ligament injury, so as to modify what was mistakenly believed, with the advent of angular stability plates, regarding the importance of early mobilization for a good functional result, what seemed to be obtainable thanks to angle stability plates.
Perhaps the most striking aspect over the past 10 years, precisely with the rapid evolution and spread of arthroscopic techniques, has been the tendency to increasingly reduce the need for classic surgical approaches. In practice, a complex fracture can be treated today with combined approaches (volar and dorsal, less invasive) thanks to the shapes of the latest generation plates, or with only volar approaches (“volar plate pre-setting”) and to obtain a reduction, as anatomical as possible, of the articular surface with arthroscopic assistance and then complete a stable fixation with mini-plates or screws, or even with only “headless” screws, through minimally invasive accesses or inserted percutaneously. Are we developing an “beyond the plate” fixation model ?. It would seem that in some situations that screws, if properly applied, can actually replace a plate. (https://chirurgiadellamanobrescia.it/atlas-on-drfs/)
Another aspect to be highlighted is the evolution of Traction Systems that can facilitate wrist fracture treatment throughout its process. From the initial diagnosis and better understanding of the “fracture model” ( under local anesthesia, before performing a temporary or definitive cast) that only a “stress view” with the Traction Tower can immediately reveal, to the reduction options available on the operating table, both in horizontal and in vertical traction, which can undoubtedly facilitate the reduction of complex metadiaphyseal, volar and dorsal fragmentation, or fragmentation of the articular surface, and make arthroscopic applications more and more frequent and justified by the experience that a surgeon acquires following the necessary learning curve.
And the challenge towards a Guideline that can help the surgeon, with the latest concepts on associated extrinsic and ixtrinsic ligament injuries, without closing him in a rigid system but looking like a “recommended” path to follow in order to identify the best strategy for treating a wrist fracture, continues…
References
Putnam MD, Fisher MD. Treatment of unstable distal radius fractures. J Hand Surg, 22A:238,1997.
Lindau T, Arner M, Hagberg L. Intraarticular lesions in distal fractures of the radius in young adults. A descriptive arthroscopic study in 50 patients. J Hand Surg [Br] 1997; 22 (05) 638-643.
Atzei A, Borelli PP, Luchetti R. Approccio razionale alle fratture di polso. Gruppo di studio sulle Patologie del Polso. SICM 2002.
Luchetti R, Papini-Zorzi I, Atzei A, Borelli PP. Ruolo dell’artroscopia nel trattamento delle fratture di Radio. Riv Chir Mano – Vol. 43 (3) 2006.
del Piñal F, Editor; Mathoulin C, Luchetti R, Co-Editors. Arthroscopic Management of Distal Radius Fractures. Springer-Verlag Berlin Heidelberg, 2010.
Atzei A. Arthroscopic Management of DRUJ Instability Following TFCC Ulnar Tears. In del Piñal F., Editor; Mathoulin C., Luchetti R., Co-Editors.
Arthroscopic Management of Distal Radius Fractures. Chapter 6. Springer-Verlag Berlin Heidelberg, 2010.
Arora R., Gabl M., Lutz M. Aspects of Current Management of Distal Radius Fractures in the Elderly Individuals. Geriatric Orthop Surg Rehabil. 2011 Sept-Nov: 2(5-6).
Mandziak DG, Watts AC, Bain GI. Ligament contribution to patterns of articular fractures of the distal radius. J Hand Surg Am 2011;36 (10):1621–1625
Borelli PP, Atzei A, Luchetti R. Proposta di un algoritmo di trattamento delle fratture di polso: 10 anni di esperienza. Rivista di Chirurgia della Mano, Vol. 49 (2) 2012.
Bain G, Alexander J, Eng K et al. Ligament origins are preserved in distal radial intraarticular two-part fractures: a computed tomography-based study. 2013 J Wrist Surg 02:255–262.
Herzberg G. Acute Distal Radius Fracture: PAF Analysis. J Wrist Surg, 2013.
Brink PRG, Rikli DA. Four-Corner Concept: CT-Based Assessment of Fracture Patterns in Distal Radius. J Wrist Surg, 2016; 147-152.
Bain G, McLean S, McNaughton T, Williams R. Microstructure of the distal radius and its relevance to distal radius fractures. 2017 J Wrist Surg 06:307–315.
del Piñal F. Atlas of Distal Radius Fractures. Thieme Ed., 2018.
Kaiser P, Gruber H, Schmidle G, Arora R, Gabl M. Positioning of a Volar Locking Plate with a Central Flexor Pollicis Longus Tendon Notch in Distal Radius Fractures. J Wrist Surg, 2019; 8:482-489.
Aita MA, Kaempf de Oliveira R, Mantovani Ruggiero G, Miller Reis RL. Bridging versus Nonbridging Dynamic External Fixation of Unstable Distal Radius Fractures in the Elderly with Polytrauma: A Randomized Study. J Wrist Surg 2019, 8: 408-416.
Schuind F. Is there a role for External Fixation with or without Kirschner Wires? In del Piñal F (Editor –in-Chief), Haerle M, Krimmer H (Co-Editors). Distal Radius Fractures and Carpal Instabilities. FESSH/IFSSH 2019 Instructional book. Thieme.
MacLean S., Bain G. Anatomy of the Fracture. in Distal Radius Fractures and Carpal Instabilities. FESSH/IFSSH 2019 Instructional book. Thieme.
Biondi M, Keller M, Merenghi L, Gabl M, Lauri G. Hook Plate for Volar Rim Fractures of the Distal Radius: Review of the First 23 Cases and Focus on Dorsal Radiocarpal Dislocation. J Wrist Surg, 2019; 8:93-99.
Biondi M, Lauri G. Dorsal fracture-dislocation of the radiocarpal joint: a new classification and implications in surgical treatment. Volume 45, Issue 7 of Journal of Hand Surgery (European Volume) 2020.
Shigi A, Oka K, Kuriyama K, Tanaka H, Yoshikawa H and Murase T. Three-dimensional analysis of displacement characteristics of dorsally angulated intra-articular distal radial fractures Journal of Hand Surgery (European Volume) 2020, Vol. 45(4):339–347.
Hintringer W, Rosenauer R, Pezzei C, Quadlbauer S, Jurkowitsch J, Keuchel T, Hausner T, Leixnering M, Krimmer H. Biomechanical considerations on a CT‐based treatment‐oriented classification in radius fractures. Archives of Orthopaedic and Trauma Surgery. 2020
Biondi M, Poggetti A, Fagetti A,Di Maro A, Bigazzi P, Pfanner S, Lauri G. Fragment specific fixation with APTUS wrist system for volar rim fractures of the distal radius: a multicentric study. European Journal of Trauma and Emergency. Surgery 2021
Eardley-Harris N, MacLean S, Jaarsma R, Clarnette J, Bain GI. Volar Marginal Rim Fractures of the Distal Radius Have a Higher Rate of Associated Carpal Injuries – A Comparative Cohort Study. JWS 2021
How many Sets do you need in your operating room to fix a Distal Radial Fracture?

La proposta dell’algoritmo di trattamento delle fratture di Polso, dopo 10 anni di implementazione congressuale, è stata pubblicata nella Rivista di Chirurgia della Mano della SICM nel 2012 ( scarica il Pdf ). I 10 anni, dal 2002 al 2012, sono stati caratterizzati dai sistemi di placche volari a stabilità angolare, che lentamente si sono evolute dall’angolazione fissa all’angolazione variabile poliassiale. Cosa è cambiato negli ultimi 8 anni?
L’esame TAC, che orienta sempre di più, in ogni sistema classificativo, il trattamento di una frattura di polso che presenta i segni radiologici di instabilità, si è arricchita di nuove tecnologie come la TAC “cone beam”, derivata dalla applicazione in ambito maxillo-facciale. La TCCB sta sostituendo sempre più la TC tradizionale in distretti anatomici come il polso e la mano, e grazie alla emissione di radiazioni ionizzanti sempre più basse ma alla risoluzione sempre più alta, spesso può sostituire il radiogramma tradizionale quando si deve interpretare meglio un conflitto osseo o un “gap” o un “decalage“ articolare o un processo di consolidazione in evoluzione.
La RM con le nuove macchine ad alto campo ( 1,5 3T ) rimane il gold standard nella diagnostica delle lesioni legamentose associate.
I fissatori esterni hanno mantenuto il loro ruolo di nicchia, e si sono evoluti nella direzione di kit sterili monouso e nella semplicità del montaggio (1 solo strumento per il montaggio di tutti gli elementi).
La “spanning plate”, ( definita anche placca a ponte o placca in distrazione o Fissatore Interno ) sempre più utilizzata nelle fratture articolari con comminuzione severa e marginale, nei politraumatizzati con fratture bilaterali, si è affiancata al ringiovanito FE, e compete con questo per offrire una maggior stabilità con una distrazione articolare minima ( si riduce la percentuale della nota algodistrofia secondaria ) e per eliminare il problema dell’infezione delle fisches soprattutto quando il processo di consolidazione richiede un tempo superiore ai 3 mesi ( osso osteoporotico degli anziani ). La scelta rimane comunque ancora chirurgo dipendente.
Ma è soprattutto curioso notare come vi sia stato un ritorno al concetto della FSF ( Fragment Specific Fixation ) che già aveva caratterizzato la sintesi delle fratture di polso negli anni 90, ovvero sempre più diretti verso una riduzione stabile sempre più anatomica dei singoli frammenti e con più accessi chirurgici, volari, combinati o dorsali. Negli ultimi anni i set chirurgici si sono arricchiti man mano di placche di varie dimensioni e morfologia, con uncini incorporati all’estremità distale e di “uncini” sempre più dedicati alle variabili dimensioni dei frammenti marginali, con la finalità di una sintesi sempre più dedicata ai frammenti “chiave” ( “key fragments”, frammenti con connessioni legamentose ) della frattura, ovvero a quei frammenti che danno stabilità all’intero montaggio e quindi al polso nel suo insieme. La sfida per il mercato si è rivolta verso la ricerca di un Sistema di mezzi di sintesi il più completo possibile, che possa gestire in modo stabile tutti i frammenti di ogni dimensione di una frattura complessa. La sfida è ancora aperta anche se dobbiamo riconoscere ad alcuni Sistemi, tra cui quello rappresentato nell’algoritmo, di aver forse completato il “puzzle” di elementi in grado di affrontare le variabili di rappresentazione delle fratture di radio e ulna distali.
Non dobbiamo tuttavia dimenticare la variabile delle lesioni legamentose associate alle fratture del polso dove il ruolo dell’artroscopia diagnostica e chirurgica è cresciuto, giustificando la necessità per un chirurgo di approfondire la sua esperienza e le sue conoscenze nell’applicazione di questa tecnica. L’argomento tuttavia rimane a tutt’oggi controverso, con la posizione di alcuni chirurghi esperti che non ritengono necessario il controllo artroscopico di una riduzione anatomica o la sintesi con assistenza artroscopica in una frattura intra-articolare o la conferma di una lesione legamentosa associata. Per i legamenti interossei della prima filiera, ad esempio, è il decorso particolare di una rima di frattura sul radiogramma standard che fa sospettare una lesione legamentosa e che va approfondito con esami radiologici dinamici (stress view in trazione o fluoroscopia dinamica) preoperatori o eseguiti una volta terminata la sintesi; per il complesso legamentoso TFCC, invece, si può ricorrere a test clinici (test del ballottamento) pre-operatori o più frequentemente una volta eseguita la sintesi stabile del radio distale.
Tuttavia l’artroscopia è strumento diagnostico di elevata attendibilità per quantificare lesioni legamento parziali (che non si evidenziano con le manovre in precedenza citate) e per i danni osteo-cartilaginei superficiali (non evidenti ai radiogrammi standard). Se le prime hanno capacità di guarigione spontanea, gli altri, se non rimossi, possono generare corpi liberi endoarticolari e comunque essere la sede per lo sviluppo di un’artosi secondaria. Infine le informazioni ricavate dal controllo artroscopico sono utili per adattare il percorso riabilitativo postoperatorio al necessario tempo richiesto dalla guarigione della lesione legamentosa associata: così da modificare quello che si riteneva erroneamente, con l’avvento delle placche a stabilità angolare, riguardo l’importanza della mobilizzazione precoce, consentita dalle caratteristiche del mezzo di sintesi, per un buon risultato funzionale.
Ma l’aspetto forse più eclattante di questi ultimi 10 anni, proprio con il rapido evolversi e diffusione delle tecniche artroscopiche, è stata la tendenza a ridurre sempre più la necessità degli accessi chirurgici classici. In pratica una frattura complessa può essere trattata oggi con accessi combinati, volari e dorsali, sempre meno invasivi, grazie alla morfologia delle placche di ultima generazione, oppure con il solo accesso volare ( volar plate pre-setting ) per poi ottenere la riduzione, la più anatomica possibile, della superficie articolare con l’assistenza artroscopica e terminare la sintesi con mini-placche o semplicemente viti, oppure addirittura con le sole viti “headless”, attraverso accessi mini-invasivi o addirittura inserite per via percutanea. Stiamo in pratica arrivando ad un modello di sintesi “over the plate ?”. Sembrerebbe che in alcune situazioni le viti, se appropriatamente applicate, possano in effetti sostituire una placca. (https://chirurgiadellamanobrescia.it/atlas-on-drfs/ )
Un altro aspetto da sottolineare è rappresentato dall’evoluzione dei sistemi di Trazione che possono agevolare il trattamento di una frattura di polso per tutto il suo percorso.
Dalla diagnostica iniziale (direttamente in sala gessi, in anestesia locale, prima della eventuale confezione di stecca gessata temporanea o apparecchio gessato definitivo) di un modello di frammentazione che solo una “stress view” su Torre di Trazione può immediatamente svelare, fino alle manovre riduttive praticabili al tavolo operatorio, sia in Trazione Orizzontale che Verticale, che possono indubbiamente agevolare la riduzione di frammentazioni complesse meta-diafisarie, volari e dorsali, e di frammentazioni della superficie articolare, e rendere il gesto artroscopico sempre più frequente e giustificato dall’esperienza che il chirurgo acquisice secondo la necessaria curva di apprendimento.
E la sfida verso una Linea Guida che possa aiutare il chirurgo, senza chiuderlo in un Sistema rigido e chiuso, ma che suoni come una “raccomandazione” da seguire per individuare la migliore strategia di trattamento di una frattura di polso, continua.